




























テキスト全文
- #1.
59 yo female A case of bilateral nosebleeds while being treated for pneumonia Hirotake Mori h.mori.oa@juntendo.ac.jp Department of General Medicine Faculty of Medicine, Juntendo University
- #2.
Case: 59yo female Chief complaints: fever, cough Present Medical History: The patient presented to the hospital with a fever and persistent productive cough that began 4 days prior. Childhood history was significant for recurrent bilateral nosebleeds. A diagnosis of allergic rhinitis had been previously made by ENT.
- #3.
Past Medical History: gastric ulcers, nosebleeds Medication: - Nizatidine (150mg) 2 tablets PO bid (after meals, morning, evening) - Fexofenadine (60mg) 2 tablets PO bid (after meals, morning, evening) Lifestyle: social drinker, non-smoker Allergy: none Family History: Mother: surgical resection of the lungs for pulmonary AVM Eldest daughter: x-ray of the chest revealed abnormal lung shadows during a routine health maintenance visit.
- #4.
Physical Examination Height: 162cm Weight: 39kg Vital signs: BP 138/58mmHg, HR 97bpm, RR 20/min, SpO2 91%, BT 37.9℃ Face: ulcerations in the perioral region Chest: auscultation of the posterior chest revealed coarse crackles at the left lower lung field. Abdomen, extremities: no abnormalities
- #5.
Laboratory Test Results <CBC> WBC <Metabolic Panel> 4.7 ×103/mL Na 134 mmol/L Nt 93.5 % K 3.6 mmol/L Ly 4.7 % Cl 97 mmol/L Hb 14.6 g/dL AST 56 U/L Ht 43.3 % ALT 25 U/L MCV 90.4 fL T-Bi 1.4 mg/dL MCH 30.6 pg BUN 55 mg/dL Plt 182 ×103/μL Cr CRP <Urine Rapid Antigen Test> Urine legionella (-) Urine pneumococcus (+) *unable to obtain sputum sample* 1.23 mg/dL 42.03 mg/dL WBC left shift, abnormal LFT / kidney function, and high CRP
- #6.
X-ray of the Chest
- #7.
CT Scan of the Chest CT scan revealed hyperdense infiltrate in the left lung accompanied by air bronchograms. Diagnosis was made for pneumococcal pneumonia. The patient was hospitalized, and treatment was initiated.
- #8.
Course of Hospitalization 38 37.5 37 36.5 36 35.5 1 2 3 4 5 6 7 8 9 10 11 12 13 CTRX 2g/day AZM 500mg/day O2 admin. 1L CRP (mg/dl) 42 1L 39 Discontinued 6 Pneumococcal pneumonia: breathing function, values of LFT / kidney function improved within a few days.
- #9.
Course of Hospitalization Bilateral nosebleeds 38 37.5 37 36.5 36 Ulcerations of the perioral region, nostril, soft palate, pharynx 35.5 1 2 3 4 5 6 7 CTRX 2g/day AZM 500mg/day - Ulceration was seen in the perioral region, nasal cavity, soft palate, and pharynx. - Persistent bilateral nosebleeds 8 9 10 11 12 13
- #10.
Course of Hospitalization Bilateral nosebleeds 38 37.5 37 36.5 36 Ulcerations of the perioral region, nostril, soft palate, pharynx 35.5 1 2 3 4 5 6 7 8 CTRX 2g/day AZM 500mg/day HSV Infection Acyclovir IV → Valacyclovir PO 1)Pneumococcal pneumonia 2)HSV infection 3)Bilateral nosebleeds?? 9 10 11 12 13
- #11.
Characteristics of the Nosebleed Bilateral slow, oozing bleeding intermittent course postnasal drip dried blood clot → evaluation of nasal cavity proved difficult nasal obstruction → dryness, pain in the oral cavity → loss of appetite is exacerbated. The patient’s words verbatim: “The nosebleed is the same as before…” Due to the unusual characteristics of the nosebleed, consultation with the ENT dept. was indicated.
- #12.
Telangiectasia in the nasal cavity and tongue Hereditary Hemorrhagic Telangiectasia (HHT) is suspected.
- #13.
Course of Hospitalization Bilateral nosebleeds 38 37.5 37 36.5 36 Ulcerations of the perioral region, nostril, soft palate, pharynx 35.5 1 2 3 4 5 6 7 8 9 10 11 12 13 CTRX 2g/day AZM 500mg/day HSV Infection Acyclovir IV → Valacyclovir PO - nasal irrigation was performed by ENT. 1)Pneumococcal pneumonia - Vaseline was applied for moisturization, barrier protection. 2)HSV infection - pt was discharged on day 12 after 3)HHT resolution of the nosebleeds
- #14.
Hereditary Hemorrhagic Telangiectasia (HHT) Diagnostic Criteria: ① spontaneous, recurrent epistaxis ② mucocutaneous telangiectasias characteristic locations: lip, oral cavity, nose, digits others: sclera, ear ③ presence of arteriovenous malformation (AVM) in the: lung, brain, liver, spinal cord, digestive tract ④ patient is a first degree relative of a family member with HHT. More than 3 criteria → definitive diagnosis More than 2 criteria → suspected diagnosis
- #15.
no remarkable AVM was revealed
- #16.
Eldest daughter 34yo female The patient’s daughter presented to the outpatient for further investigation of the abnormal lung shadows that was revealed during a previous health maintenance visit. The daughter was referred to the university hospital for evaluation of the pulmonary AVM, genetic testing, and treatment.
- #17.
Hereditary Hemorrhagic Telangiectasia (HHT) Diagnostic Criteria: ① spontaneous, recurrent epistaxis ② mucocutaneous telangiectasias characteristic locations: lip, oral cavity, nose, digits others: sclera, ear ③ presence of arteriovenous malformation (AVM) in the: lung, brain, liver, spinal cord, digestive tract ④ patient is a first degree relative of a family member with HHT. More than 3 criteria → definitive diagnosis More than 2 criteria → suspected diagnosis ①②④ → 3 criteria were satisfied for a definitive diagnosis.
- #18.
<Considerations> Hereditary Hemorrhagic Telangiectasia (HHT) Prevalence 1:5000~1:8000 Otolaryngol Clin N Am 51 (2018) 237–254 Many patients with the disorder remain undiagnosed. Although HHT affects multiple organ systems, epistaxis is the most common presenting symptom, and patients are usually referred to ENT. As such, many internal medicine specialists do not get the opportunity to encounter this disorder in clinical practice.
- #19.
Hereditary Hemorrhagic Telangiectasia (HHT) Autosomal Dominant Inheritance Type 1 Gene ENG (Endogolin) Ch Freq(%) 9 2 ACVRL1 12 61 37 18 2 (activin A receptor type II-like 1 gene) MADH4 3,4 5q and 7p These genes code for membrane proteins involved in the TGF-β signal transduction pathway found in epithelial cells. Otolaryngol Clin N Am 51 (2018) 237–254
- #20.
Hereditary Hemorrhagic Telangiectasia (HHT) Diagnostic Criteria: Curaçao Criteria for HHT Criteria 1. 2. 3. 4. epistaxis telangiectasia AVM family history Description - spontaneous, recurrent - characteristic region: perioral region, oral cavity, digits, nose - organ involvement: digestive tract, lung, liver, brain, spinal cord History of HHT within first degree relatives Definitive: 3 or more findings Suspected: 2 findings HHT unlikely: 1 or no findings The diagnostic criteria are closely linked to the genetic profile of the disorder. J Med Genet published online June 23, 2009.
- #21.
Clinical signs, Disease Freq.(%) Nosebleeds 95 GI bleeds 20 AVM Lung 50 Liver 30 Central nervous system 10
- #22.
Int J Womens Health. 2017; 9: 373–378.
- #23.
Otolaryngol Clin N Am 51 (2018) 237–254
- #24.
Hereditary Hemorrhagic Telangiectasia (HHT) Treatment, Preventive Measures Epistaxis moisturization (barrier protection), coagulation, surgical intervention → invasive procedures have the risk of worsening epistaxis and/or rupture of the nasal septum. Lung Arteriovenous Malformation Risk of heart failure Risk of brain abscess / infarct that is caused by the shunt → consider minimally invasive catheter procedures, surgical intervention, prophylactic antibiotics → scuba diving must be avoided. J Med Genet published online June 23, 2009.
- #25.
The Significance of Early Detection / Diagnosis Eldest daughter 33yo female When the daughter was 25yo, she reported dizziness and numbness after scuba diving in Phuket island, Thailand. She was admitted to a local facility, but no diagnosis was made in Thailand. Recent investigations revealed an old (previous) cerebellar infarct.
- #26.
Conclusion While being treated for pneumonia, the patient complained of bilateral nosebleeds and was diagnosed with Osler-Weber-Rendu disease (hereditary hemorrhagic telangiectasia, HHT). Telangiectasia in the nasal cavity and tongue was found. HHT was suspected. The patient’s eldest daughter was also found to have a pulmonary AVM. Further investigation revealed an old brain infarct that was caused by scuba diving. With appropriate treatment and prophylactic measures, complications that arise from the disorder can be well controlled. A young patient presenting with bilateral nosebleeds may be suggestive of HHT.
59 yo female A case of bilateral nosebleeds while being treated for pneumonia
順天堂大学医学部総合診療科学講座/マヒドン大学熱帯医学部・医学部
森博威さんの他の投稿スライド
このスライドと同じ診療科のスライド
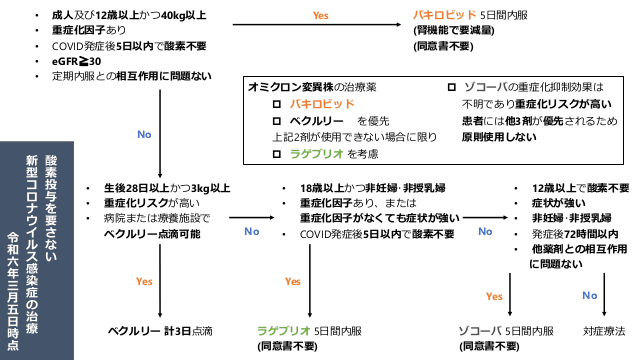
2024.4.18時点のCOVID治療薬と濃厚接触者の就業制限の考え方とワクチンまとめ
#COVID-19
4,493
1,429,449
最終更新:2024年4月18日
劇症型溶血性レンサ球菌感染症について
#連鎖球菌 #劇症型溶血性レンサ球菌感染症 #侵襲性A群連鎖球菌感染症 #iGAS #STSS
53
12,136
最終更新:2024年4月18日
新型コロナワクチン COVID-19ワクチン 2024年4月~
#感染症科 #感染症 #ワクチン #COVID
20
9,076
最終更新:2024年4月3日
抗真菌薬まとめ ver.7
#研修医 #抗真菌薬 #感染症 #カンジダ #アスペルギルス #クリプトコッカス
1,089
193,333
最終更新:2024年3月31日
2024.3.21更新 よくみる感染症のポイントをまとめました。
#抗菌薬 #感染症 #初期研修医 #原因菌
542
49,182
最終更新:2024年3月21日
地獄の内科系専門医試験を振り返よ!総合内科専門医試験向け〜感染症編〜
#内科 #総合内科専門医試験 #内科専門医試験
151
48,204
最終更新:2024年3月19日
診療科ごとのスライド
内科(538)
消化器内科(69)
循環器内科(91)
呼吸器内科(135)
血液内科(37)
糖尿病内分泌代謝内科(69)
腎臓内科(51)
アレ膠リウマチ内科(51)
脳神経内科(115)
総合診療科(234)
救急科(432)
外科(39)
消化器外科(4)
呼吸器外科(38)
乳腺外科(0)
整形外科(92)
脳神経外科(23)
泌尿器科(25)
形成外科(24)
皮膚科(35)
眼科(19)
耳鼻咽喉科(14)
歯科口腔外科(9)
リハビリテーション科(12)
心臓血管外科(8)
小児科(66)
産婦人科(52)
精神科(73)
放射線科(88)
麻酔科(14)
緩和ケア科(29)
感染症科(230)
産業医(9)
初期研修医(526)
医学生(60)
その他(368)