


























テキスト全文
- #1.
Yoshikazu Mutoh
- #2.
74yo man Nationality: Japanese Past medical history: pulmonary TB (during childhood, untreated) Medication: none Occupation: printing business (until 10y ago), currently homeless Allergy: not identified Smoking: 20 /day, quit 10y ago Alcohol: none Recent travel history: none At 9am on the day of admission, the patient is discovered fallen on the ground in the streets of Shinjuku. EMS is promptly contacted. The patient mentions losing muscle strength at 5am, from which point he is unable to move. On admission, the patient is febrile with signs of multiorgan failure, and elevated CK. An infection of unknown origin is suspected, and he is referred to our facility for consultation.
- #3.
Physical Exam on Admission Consciousness: alert BT:39.9℃ HR: 117bpm BP:100/44mmHg SpO2: 98% (RA) Head, Neck:scleral icterus • no jugular vein distention, no oral mucosa dryness, no redness of the pharynx, no oral thrush Chest: clear breathing sounds Abdomen: flat, soft. normal peristaltic sounds, no hepatosplenomegaly Back: no CVA tenderness Extremities: no edema • skin eruptions (resolved the following day) • left foot/heel pain upon applying pressure Neurological: no apparent paresis, no sensory disturbance
- #4.
Laboratory Values on Admission Alb 3.2mg/dl T.Bil 1.3mg/dl UA 2.9mg/dl BUN 122.9mg/dl Cre 5.11mg/dl AST 272IU/l ALT 153IU/l LDH 675IU/l CK 6134 mg/dl ALP 331IU/l γ-GTP 62IU/l CRP 16.02mg/dl Na K Cl Ca HbA1c PCT Influenza Rapid Antigen Test: negative 55.60ng/ml WBC RBC Hgb Hct MCV PLT 135mEq/L 3.9mEq/L 93mEq/L 8.0mg/dl 6.0% PT PT% APTT FDP 11.9sec 99.5% 28.3sec 8.9 ug/dl 15030 /mm3 Urinalysis 1.013 366 ×106/mm3 pH 1+ 10.9 /mm3 protein 30.3 % occult blood 3+ 82.8 fl 3.9 ×104/mm3
- #5.
ECG on admission: Sinus rhythm No ST segment abnormalities Echocardiography on admission: EF60.0% IVC12.0mm MR trivial TR mild PR trivial pericardial effusion(mild) Rt-pleural effusion Plain Chest X-ray on Admission
- #6.
What is the assessment? What is the plan?
- #7.
#1 1-1 1-2 1-3 1-4 Fever Thrombocytopenia Disturbance in liver function, elevated billirubin (Direct) Elevated CK Acute kidney failure #2 Skin eruptions (resolved within 1-2d) #3 History of pulmonary TB (untreated) The Differential: • Rhabdomyolysis, necrotic fasciitis, acute myocarditis, Weil disease (leptospirosis), influenza, viral hepatitis, meningitis, Dengue fever, staphylococcal septicemia • Non-infectious: TTP, myeloproliferative disorders, etc.
- #8.
Blood culture: 1 out of 2 sets CNS (coagulase negative staphylococcus) Sputum culture: negative (acid fast bacteria, common pathogenic bacteria) Urine culture: negative (acid fast bacteria, common pathogenic bacteria) Chest, abdominal CT: • slight TB shadow, infiltrative shadow on lung posterior wall • mild cardiomegaly / pericardial effusion • no abnormalities on the abdominal CT scan. Cerebrospinal fluid: not examined Skin biopsy: not taken
- #9.
Bilirubin 9 Liver Function Test 300 8 250 7 6 200 5 150 4 3 100 2 50 1 0 0 T-Bil D-Bil AST CK 10000 9000 8000 Plt 35 30 7000 25 6000 20 5000 4000 15 3000 10 2000 1000 0 5 0 ALT
- #10.
Patient history is significant for homelessness, and he mentions eating spoiled food recently. His living condition is also significant for rat sightings - leptospirosis (Weil disease) is suspected. On day 2 of hospitalization, he is started on CTRX 2g/q24h. Subsequent blood tests reveal slow but convincing improvement. On day 10, CTRX administration is ceased. On day 14, the department of infectious diseases confirms negative blood and urine PCR test results for Leptospira. No inconsistencies were found regarding the diagnosis of leptospirosis, and the case is reported to the relevant authorities. On day 16, the patient is transferred to a different facility after the results of the blood test was found clear of any abnormalities.
- #11.
Leptospirosis is a quintessential zoonotic infection that occurs worldwide, mainly in Asia and Africa. Japan faces about 20~40 cases per year, most of which originate from abroad (and become symptomatic after returning to Japan) and from recreational activities near river banks. A few hundred cases are reported among travelers. Worldwide, an estimated 1 million cases and 60,000 deaths are reported every year. International Leptospirosis Society Scientific Meeting October 7-10th, 2015 Am. J. Trop. Med. Hyg., 99(1), 2018, pp. 127–135
- #12.
The incubation period of Leptospira is around 2~16days (average 5~10days), and the urine of infected wild / domestic animals serves as its reservoir. The route of transmission is by direct contact with the infected animal or soil / water that has been contaminated by animal urine. Skin transmission is more common than oral transmission, and it is known to be transmitted via open wounds. Studies have shown that saliva causes the inactivation of the organism via linear agglutination. Leptospira has been reported in: Southeastern Asia, South Asia, Oceania, the Caribbean, Africa, and Latin America. In these regions, exposure to freshwater bodies poses the risk of infection. Additionally, outbreaks have been reported in urban areas after heavy rain. In Southeastern Asia, mass outbreaks have been reported after recreational water activities and triathlon events that involve swimming. Clin Infect Dis . 2002 Jun 15;34(12):1593-9.
- #13.
Fever Lethargy Myalgia Conjunctival hyperemia Loss of appetite Headache Hepatosplenomegaly Jaundice Cough Nausea Vomiting Bloody sputum Abdominal pain Diarrhea Lymphadenopathy Skin Eruptions 100% 100% 40-100% 28-97% 46-92% 70-98% 15-83% 1.5-95% 20-57% 29-75% 18-69% 9-37% 26-43% 11-36% 19-49% 0-7% Only 10~20% of infected patients are symptomatic. In 90% of cases, the infection does not progress to severe illness. Severity is determined by bacterial load, blood type, and immune function. Many cases are self-limiting. Leptospirosis. CLINICAL MICROBIOLOGY REVIEWS, Apr. 2001, p. 296–326 Cachay and Vinetz JPGM 51:174, 2005
- #14.
Characteristic laboratory results include: elevated bilirubin (direct > indirect; in some cases over 20mg/dl), mild elevation of liver transaminases (usually under 200IU/L), and CK elevation. If liver complications are observed, it is important to consider viral hepatitis as a possible differential. Risk factors not only include exposure to soil / water that has been contaminated by rodent urine, but also occupational risks such as: outdoor / recreational water activities, water sanitation facilities, and civil engineering / construction. Non-occupational environmental risks include: low socioeconomic status, close proximity to a garbage disposal facility, and the presence of rats near living quarters. Outbreaks have been reported during the rainy season and after floods / typhoon. Dechet AM, Parsons M, et al. January-February 2005. PLoS One. 2012; 7(7): 39672. Reis RB, Ribeiro GS, Felzemburgh RDM, Santana FS, Mohr S, et al. PLoS Negl Trop Dis 2(4): e228. An investigation revealed tha
- #15.
This finding usually appears 1-3d after the onset of symptoms and can be easily overlooked. It is seen in 27~ 93% of cases. A hyperemic conjunctiva spanning the palpebral and scleral surface is characteristic for Leptospirosis. It may progress to anterior uveitis after the resolution of the acute period. Loss of visual acuity is a chronic complication that may persist for more than 20 years according to some reports. Ocular Manifestations of Leptospirosis. J postagrad Med 2005;51:189-194
- #16.
Conjunctival hyperemia is present in 55-92% of cases but resolves during the early period of infection. Although it is a characteristic finding, it is often missed. Chu KM, Rathinam R, Namperumalsamy P, Dean D.J Infect Dis 1998;177:1314-21. Erythema / pain in the trunk and anterior tibia region (Pretibial Fever) is another characteristic finding that is present in 10% of cases. Mohammed, H., C. Nozha, K. Hakim, F. Abdelaziz and B. Rekia, 2011. Bacteriol. J., 1:1-7.
- #17.
This finding is present in 10% of cases. Faint-colored erythema can be seen on the trunk, umbilical region, and over the muscles of the extremities, and it usually resolves within the first few days of infection. It is known as Fort Bragg Fever. Also known as Pretibial Fever, it only develops a few days after the onset of symptoms. Tenderness is felt when pressure is applied on the gastrocnemius. Leptospirosis Caused by Serotype fort-Bragg: A Suburban Outbreak. Ann Intern Med. 1973;79(6):786-789.
- #18.
Leptospirosis can be diagnosed using four methods: 1. Direct microscopic investigation 2. Leptospira culture isolation using a specialized growth medium 3. Serology 4. Leptospira genetic PCR analysis
- #19.
Influenza Hantavirus TTP Pharyngitis Dengue fever Hemolytic uremic syndrome Aseptic meningitis Malaria Antiphospholipid syndrome Acute HIV infection Typhoid / Parathyphoid fever Rhabdomyolysis Viral hepatitis Rickettsiosis Acute pancreatitis Legionellosis Viral hemorrhagic fever
- #20.
Outpatien t Doxycycline 100mg twice /day for 7d Azithromycin 500mg once /day for 3d ※under 8yo or pregnant women: Azithromycin (pediatric: 10mg/kg once / day) or Amoxicillin (25-50mg/kg in 3 doses) Severe cases that received Penicillin G 8 million units / day for 5d reported no difference in treatment period in comparison to the control group. UpToDate:Nov 20, 2014.
- #21.
Avoid contact with contaminated bodies of freshwater, rodents, and other animal carriers. Wear protective gear such as rubber gloves, boots, and goggles – walking barefoot is a risk factor. An inactivated vaccine has demonstrated some degree of efficacy in dogs, cats, and pigs, but the efficacy in humans remains uncertain as it undergoes clinical trials.
- #22.
A regimen of prophylactic antibiotics is recommended when exposure to environmental risks is unavoidable. Its effectiveness was demonstrated among military personnel undertaking exercises in the jungle. Prophylaxis prevented many of the symptoms seen throughout the body, but it showed no significant difference in outcome between the asymptomatic infection group and the control group. Adverse effects of doxycycline include daylight sensitivity and GI disturbance. It is contraindicated in pregnancy and children. Mandell, Douglas, and Bennett's principles and practice of infectious diseases. 8th ed. 2015:2714-2720.
- #23.
As a category IV infection, Leptospirosis must be reported to the relevant authorities. Up until the 1970’s, 50 lethal cases were reported every year. In recent years, an average of 30-50 cases are reported annually, which originate from within Japan. Over half of these cases are reported in Okinawa. In 2022, the first lethal case in 16 years was reported (Okinawan man in his 70’s). Exposure risks include: • Agriculture-related exposure to contaminated water. • Recreational activities near bodies of freshwater (river, lakes) • Exposure to rat urine in urban areas following typhoon-related heavy rain. (人) 80 70 60 50 40 About 20-50 cases of Leptospirosis among pet dogs have been reported annually. 30 20 10 0 2014 2015 2016 2017 2018 2019 2020 2021 2022 https://idsc.tmiph.metro.tokyo.lg.jp/diseases/leptospirosis/ https://www.pref.okinawa.jp/site/hoken/vaccine/yobou/press/documents/20221017_leptospira.pdf
- #24.
Leptospirosis is a febrile disease that occurs mainly from exposure to contaminated water (freshwater) and is localized in Southeast Asia / other tropical regions. Although it is relatively rare in Japan, one may consider Leptospira as a differential if the patient history is significant for overseas travels or possible exposure to rat urine in urban areas. If the disease is not in the clinical scope, diagnosis can be challenging. However, Leptospirosis is relatively straightforward to identify if these major clues are recognized: freshwater exposure, recent heavy rainfall (typhoon season), and fever + jaundice. Only specialized facilities have the capacity to identify Leptospira, and this can be a limiting factor in the diagnostic process. It may be helpful to know if any of these facilities are accessible near your place of practice.
A Case of Fever in the Mertopolitan Area
公立陶生病院
武藤義和さんの他の投稿スライド
このスライドと同じ診療科のスライド
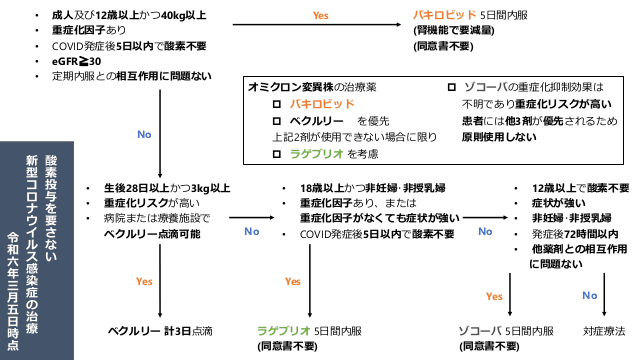
2024.4.18時点のCOVID治療薬と濃厚接触者の就業制限の考え方とワクチンまとめ
#COVID-19
4,493
1,429,366
最終更新:2024年4月18日
劇症型溶血性レンサ球菌感染症について
#連鎖球菌 #劇症型溶血性レンサ球菌感染症 #侵襲性A群連鎖球菌感染症 #iGAS #STSS
53
12,112
最終更新:2024年4月18日
新型コロナワクチン COVID-19ワクチン 2024年4月~
#感染症科 #感染症 #ワクチン #COVID
20
9,076
最終更新:2024年4月3日
抗真菌薬まとめ ver.7
#研修医 #抗真菌薬 #感染症 #カンジダ #アスペルギルス #クリプトコッカス
1,089
193,285
最終更新:2024年3月31日
2024.3.21更新 よくみる感染症のポイントをまとめました。
#抗菌薬 #感染症 #初期研修医 #原因菌
542
49,152
最終更新:2024年3月21日
地獄の内科系専門医試験を振り返よ!総合内科専門医試験向け〜感染症編〜
#内科 #総合内科専門医試験 #内科専門医試験
151
48,204
最終更新:2024年3月19日
診療科ごとのスライド
内科(538)
消化器内科(69)
循環器内科(91)
呼吸器内科(135)
血液内科(37)
糖尿病内分泌代謝内科(69)
腎臓内科(51)
アレ膠リウマチ内科(51)
脳神経内科(115)
総合診療科(234)
救急科(432)
外科(39)
消化器外科(4)
呼吸器外科(38)
乳腺外科(0)
整形外科(92)
脳神経外科(23)
泌尿器科(25)
形成外科(24)
皮膚科(35)
眼科(19)
耳鼻咽喉科(14)
歯科口腔外科(9)
リハビリテーション科(12)
心臓血管外科(8)
小児科(66)
産婦人科(52)
精神科(73)
放射線科(88)
麻酔科(14)
緩和ケア科(29)
感染症科(230)
産業医(9)
初期研修医(526)
医学生(60)
その他(368)